
Biohacking Sensory and Social Processing: Optimizing Integration
Your brain runs on prediction. It takes a flood of sensory input and social cues, builds a model of the world, and places you inside it. That model gets updated thousands of times a second, and it usually runs in the background where you never notice it.
These systems run differently in different people. Some of you are hypersensitive to sensory input. Noise, textures, fluorescent lights, the tag in a shirt. Others read social cues with effort instead of automatically. Sarcasm lands flat, facial expressions blur, group dynamics turn into a guessing game.
You're not imagining either of these. You're not weak for being overwhelmed in a loud restaurant, and you're not socially defective for missing a cue everyone else caught. These are differences in how your posterior (sensory) and frontal (social-emotional) networks process and integrate information. Here is the neuroscience, the QEEG signatures I see when these systems are dysregulated, and the interventions that move the dial.
How does the brain process information from back to front?
Your cortex runs a hierarchy, roughly back to front.
Occipital lobe (primary visual cortex, V1): First stop for vision. Detects edges, motion, color.
Temporal lobe (primary auditory cortex, A1): First stop for sound. Detects frequency, intensity, timing.
Parietal lobe (association cortex): The integrator. It combines visual, auditory, tactile, and proprioceptive (body position) signals into one coherent perception.
Frontal lobe (prefrontal cortex): Interprets the integrated input against your goals, your history, and its social-emotional meaning, then generates decisions and actions.
The flow runs from sensory input at the back of the brain, through integration in the parietal lobe, to interpretation and action up front. Each handoff can fail in its own way. Sensory areas can over-fire (hyperresponsivity). The parietal integrator can under-bind the pieces (poor gestalt formation). Frontal regulation can run weak, and then ordinary sensory load tips into overwhelm and ordinary social situations turn into confusion.
What are the social brain networks?
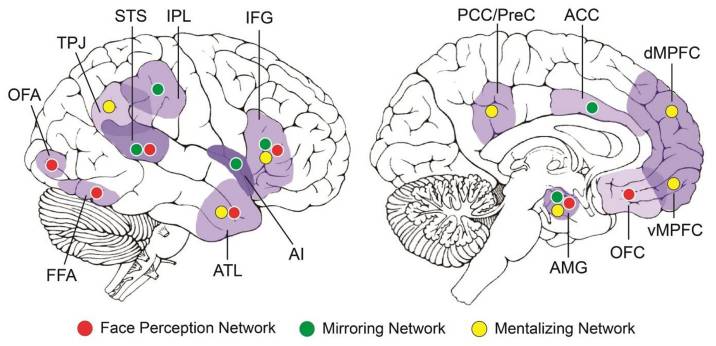
Social cognition isn't one region. It's several networks running in parallel: the mirror neuron system for understanding actions and intentions, a theory-of-mind network for perspective-taking, and emotional processing circuits in the amygdala, insula, and anterior cingulate.
Superior temporal sulcus (STS): Processes biological motion, walking, gesturing, facial movement, and tracks social cues like eye-gaze direction and body language.
Fusiform face area (FFA): Specialized for faces. Distinguishes individuals and reads expressions. Damage here produces prosopagnosia, the inability to recognize faces.
Temporoparietal junction (TPJ): Theory of mind, the machinery for modeling another person's beliefs, intentions, and mental states, and for seeing a situation from their viewpoint.
Medial prefrontal cortex (mPFC): Self-referential processing, social judgment, mentalizing. It overlaps with the default mode network that runs during rest.
Anterior cingulate cortex (ACC) and insula: Emotional awareness, the ability to notice your own state, plus empathy. Social pain from rejection or exclusion lights up these regions much like physical pain does.
Amygdala: Emotional salience. It flags what's threatening and what's rewarding, detects anger and fear in faces, and tunes how strongly an emotional event gets written into memory.
What do mirror neurons actually do?
Mirror neurons fire both when you perform an action and when you watch someone else perform it. They were first recorded in macaque premotor cortex in the 1990s. The human mirror system spans premotor cortex, the inferior parietal lobule, and the STS.
They let you understand an action by simulating it in your own motor system, they support imitation learning (watch, then do), and they feed empathy: watching someone in pain activates pain-related circuits in your own brain.
The mirror-neuron-dysfunction theory of autism is widely cited and genuinely controversial. Treat it as unsettled. What the imaging supports more cleanly is that autistic brains show different patterns of social activation during social tasks, not absent activation.
Why does sensory input feel too loud for some people?
Sensory processing disorder isn't a formal DSM diagnosis, but the experience is real and measurable. Some people are flooded by input that others barely register.
It runs on a spectrum. On the hyporesponsive (under-reactive) end, you seek intense input: loud music, rough textures, spicy food. You may miss pain or temperature shifts, and you can look checked out or inattentive. On the hyperresponsive (over-reactive) end, everyday input overwhelms you: clothing tags, fluorescent lights, ambient chatter. You avoid certain textures, sounds, and crowds, and you read as anxious or irritable.
The mechanism is sensory gating, your brain's ability to filter out low-priority input. Normally the thalamus and sensory cortex screen out the irrelevant so attention can land on what matters. When gating runs weak, everything arrives at full volume. That's exhausting, and it's not a discipline problem.
In the QEEG, I see a few signatures of weak gating:
- Poor alpha blocking. Alpha should suppress when you actively process a stimulus. When it doesn't drop, gating is weak. (More on this rhythm in Decoding Alpha Waves.)
- Elevated beta over sensory areas, consistent with hyperarousal and hyperresponsivity.
- Reduced SMR (12-15 Hz at the sensorimotor cortex), which tracks with poor sensory filtering.
What interventions optimize sensory and social processing?
Sensory integration therapy (occupational therapy)
For hyper- or hyporesponsivity, occupational therapy built on sensory integration principles is the standard starting point. The approach uses graduated exposure to build tolerance, proprioceptive work (heavy lifting, deep pressure) to regulate arousal, and vestibular input (swinging, spinning) to bind the sensory systems together.
The evidence is mixed. Some trials show benefit, others don't, and the effect is clearest in children. The mechanism remains poorly specified. I rate this as a reasonable first-line option for kids, weaker for adults.
Neurofeedback for sensory gating
When a QEEG shows poor alpha blocking or hot sensory cortex, neurofeedback gives you a way to train the gating directly.
SMR training (12-15 Hz at C3, C4, Cz) strengthens sensory filtering and lowers hyperresponsivity to input. Alpha training at posterior sites trains your ability to generate and suppress alpha on demand, which is the same skill as turning down irrelevant input. Plan on 20-40 sessions with gradual change rather than a switch flipping. If you want the deeper mechanism behind the calm-alert band, see SMR Neurofeedback. For whether the modality holds up generally, Is Neurofeedback Legitimate? walks through the evidence.
Meditation for sensory awareness
Meditation trains the same circuits from the inside. It builds interoception (body awareness), sharpens selective attention so you filter distractions, and lowers reactivity to sensory stimuli.
If you run hyperresponsive, body-scan meditation trains systematic attention to sensation without reacting to it, and breathing meditation anchors attention to pull you out of overwhelm. Ten to twenty minutes daily is a workable dose. If you run hyporesponsive, mindful eating, walking, or movement does the opposite job, raising your sensory resolution rather than damping it.
Social skills training plus neurofeedback
For social processing difficulties, including autism, social anxiety, and alexithymia, combined approaches outperform either piece alone.
Social skills training makes the implicit explicit. You teach facial expressions, body language, and conversational turn-taking directly, using role-play and video modeling, building conscious strategies where the automatic read is weak.
On the neurofeedback side, the right TPJ (trained at T4, T6, P4) is a candidate target for theory of mind and perspective-taking, over 20-40 sessions. Frontal targets include alpha training at Fz to lower social anxiety and beta down-training to quiet social hypervigilance. The TPJ and social-cognition targeting is closer to clinical extrapolation than established protocol, so set expectations accordingly. Social change is slow regardless of method; budget 12 to 24 weeks for anything you'd call noticeable.
Oxytocin (experimental)
Oxytocin is a neuropeptide tied to social bonding, trust, and empathy. Intranasal oxytocin improves some aspects of social cognition in some autistic individuals, reading emotions and making eye contact, but the effects are context-dependent, temporary (hours, not days), and inconsistent across studies. I don't recommend it as a primary intervention. The response depends on dose, context, and individual baseline, and it belongs under medical supervision.
Environmental modifications
The fastest wins often live in the environment, not the brain.
For sensory hyperresponsivity: noise-cancelling headphones to cut auditory load, sunglasses indoors when fluorescents are the trigger, weighted blankets for the calming pull of deep pressure, and quiet dim spaces to recover in after multisensory environments.
For social processing difficulties: structured interactions with clear roles and expectations, written communication when in-person is too much, and prepared scripts for common scenarios so you're not improvising under load.
Is autism a different operating system?
Autism is a different way of processing social and sensory information, with its own strengths and costs. The literature points to reduced spontaneous attention to social stimuli like faces and voices, increased attention to non-social structure like patterns, textures, and systems, and distinct neural activation during social tasks rather than missing activation.
The interventions that help are the same ones above, aimed at function rather than conformity: explicit social skills training that teaches consciously what neurotypical brains absorb implicitly, environmental accommodations to lower sensory load, neurofeedback for specific dysregulation when the QEEG shows a target worth training, and deliberate use of strengths like pattern recognition and systematic thinking. The aim is to reduce distress and improve function where the person wants it improved.
Bottom line
Sensory and social processing depend on distributed networks spanning the occipital lobe (vision), temporal lobe (hearing, face processing), parietal lobe (integration), and frontal lobe (interpretation, social cognition). When those systems run out of balance, you get sensory hyperresponsivity (overwhelm), hyporesponsivity (input-seeking), or social difficulty (missed cues, misread intentions).
The intervention menu:
- Occupational therapy for sensory integration, strongest in children.
- Neurofeedback, SMR for gating and right-TPJ training for social cognition.
- Meditation for body awareness and sensory regulation.
- Social skills training to make implicit rules explicit.
- Environmental modifications to lower sensory load and structure social interaction.
These systems are trainable. They don't reorganize overnight, but consistent work produces measurable change: 20-40 neurofeedback sessions, 8-12 weeks of meditation, ongoing social skills practice. Your brain is adapting to whatever you feed it right now. Pick one item from the list, run it long enough to read the result, and adjust from there.
Get new articles and brain training insights by email.
No spam, unsubscribe anytime.
Related Articles
Biohacking Brain Fog: Restoring Mental Clarity
Brain fog has a measurable electrical signature. Here's the physiology, what QEEG shows, and the interventions that restore mental clarity.
Biohacking with EEG Phenotypes: Predicting Brain Function from Electrical Patterns
EEG phenotypes are stable electrical signatures that predict how you process attention, regulate mood, and respond to neurofeedback and medication.
Biohacking Memory: Optimizing Encoding, Consolidation, and Retrieval
A neuroscientist's guide to memory: how encoding, consolidation, and retrieval work, why most "memory problems" are attention problems, and what fixes them.
About Dr. Andrew Hill
Dr. Andrew Hill is a neuroscientist and pioneer in the field of brain optimization. With decades of experience in neurofeedback and cognitive enhancement, he bridges cutting-edge research with practical applications for peak performance.
Get Brain Coaching from Dr. Hill →